What is the endovascular treatment of visceral aneurysms?
An endovascular treatment is a treatment that is carried out inside the blood vessels, using small plastic tubes that are passed through a 2-3 mm hole in the skin and blood vessel wall.
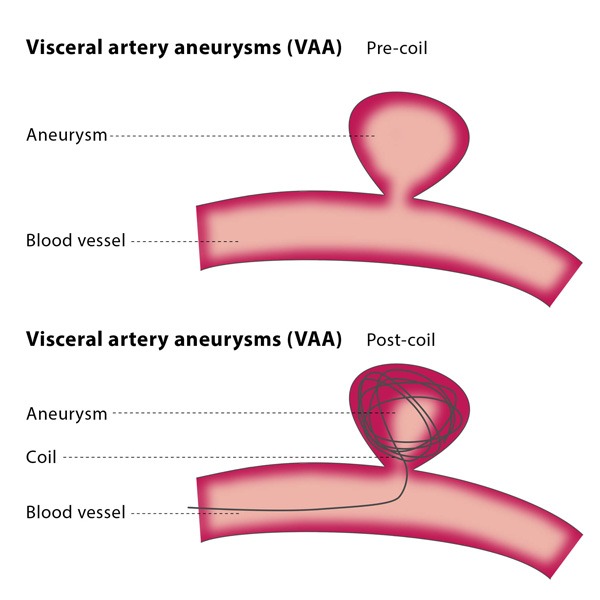
An aneurysm is an abnormal enlargement of a blood vessel. Blood vessels have a tubular structure and most of these aneurysms are blister-like enlargements. Their walls may weaken and thus have a risk of tearing or bursting.
Visceral is a collective term for an organ in your body, such as the liver or spleen, so a visceral aneurysm is an aneurysm that occurs in an organ.
These abnormal enlargements have a risk of bursting and bleeding. The typical size that indicates a need for treatment is 2 cm. Endovascular treatment aims to stop blood flow to the aneurysm while maintaining blood flow to the organ.
How does the procedure work?
If you stop blood flowing, it will clot, just like a cut to the skin. The endovascular approach aims to stop blood flowing into the aneurysm whilst also preserving flow to the organ supplied by the affected blood vessel.
The interventional radiologist will usually enter a blood vessel in your groin and guide a 2-3 mm tube to the affected blood vessel. Typically a small coil (like the spring in a pen) will be pushed into the aneurysm or else into the blood vessel supplying the aneurysm.
Alternatively a small flexible metal tube (called a covered stent) is placed over the hole that feeds the aneurysm. These techniques will cause a clot to form in the aneurysm to stop the risk of rupture.