What is an aortic dissection?
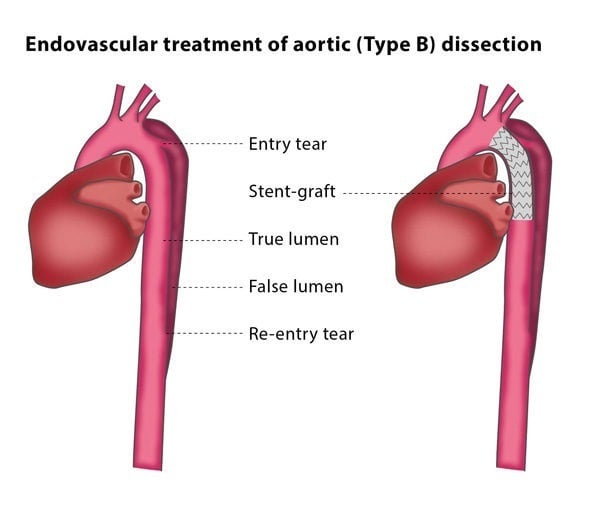
The aorta is the largest artery in your body. An aortic dissection is when the layers of the aortic wall are separated by a tear in the inner wall. The aortic wall splits into two lumens (channels): a true lumen, meaning the original lumen; and a false lumen, which is in the aortic wall. If there is high blood pressure in the false lumen, the true lumen is compressed. This decreases blood supply to the organs, leading to organ failure and restricted blood supply to the lower limbs.
There are two broad types of dissection – a tear to the artery near the heart to the point where the artery supplying the left arm takes off called Type A and a dissection beyond the origin of the artery supplying the left arm called Type B. Type A dissections need immediate surgery to repair it. Certain types of Type B dissections benefit from placement of a stent.
How does the procedure work?
The placement of a stent graft (a metallic scaffold with a surrounding fabric) is usually performed under general anaesthesia. The interventional radiologist will access an artery at the top of your leg for the procedure. They may also insert an angiography catheter through an artery in your right arm for injections of contrast material before and after the placing of the stent graft. The interventional radiologist will place a guidewire into your aortic arch and will then pass the stent graft over the wire and use this to cover the tear on the inner wall of the aorta. This protects the true lumen from the expansion of the false lumen.