How does the procedure work?
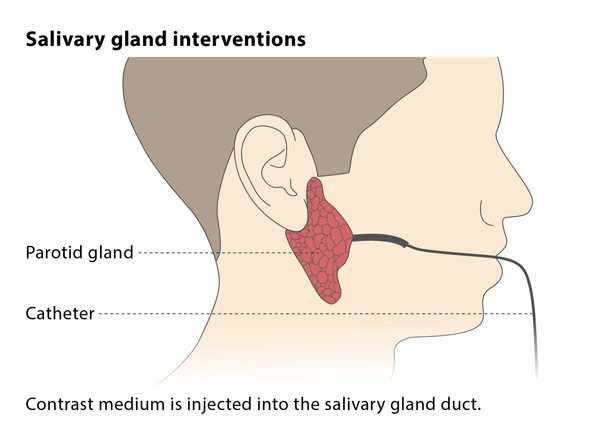
The sialoplasty procedure is carried out using X-ray guidance. An interventional radiologist will insert a catheter (a thin flexible tube) into the affected area. Before the sialoplasty procedure can be carried out, a diagnostic sialography will be performed to assess the location and extent of the condition requiring the procedure. Diagnostic sialography is an imaging technique, in which the interventional radiologist injects contrast medium (dye) into the affected salivary gland and then performs an X-ray.
During the sialoplasty, a flexible guidewire will be passed into the salivary duct and directed to the narrowed or blocked area. Using a dilator, wire retrievable basket or balloons, the interventional radiologist will then expand the narrowing of the salivary duct or extracts the stones (or both), thus relieving the cause of the condition.
Why perform it?
Interventional techniques can be used to remove stones or other causes of obstruction in the salivary glands, relieving the symptoms caused by the blockage. When stones form in the glands, patients may experience a range of symptoms including pain, swelling and infection.
It has been suggested that interventional techniques may not be a suitable treatment if the stone causing the blockage is too large. However, the number of reported cases of this is small, making it impossible to give firm recommendations for these techniques. On the whole, interventional procedures are considered safe and successful.
What are the risks?
Patients usually experience swelling following the procedure, but this does not last longer than 24-48 hours. Some patients experience a tingling sensation in the tongue, but this resolves itself with time.
The procedure carries risks of bleeding in the mouth (though this is self-limiting so does not need treatment), pain during the procedure and infection. Contrast dye may leak into the tissue around the vein in which the needle was placed, or the doctor may accidentally create a false passage (an unnatural passage leading off from the normal duct). However, these usually do not have permanent consequences. More serious complications include ductal tears or duct detachment, which may subsequently require surgical removal of the gland.
Bibliography
1. Buckenham T M, George C D, McVicar D, Moody A R, Coles G S. Digital sialography: imaging and intervention, Br J Radiol. 1994; 67:524–529.
2. Brown JE et al. Minimally invasive radiologically guided intervention for the treatment of salivary calculi, Cardiovasc Intervent Radiol. 2002; 25:352-5.